Prostate carcinoma remains one of the most prevalent malignancies affecting the male population globally. When seeking Genitourinary Cancer Treatment in Bangalore, patients must evaluate specialized facilities that provide comprehensive, multidisciplinary care.
As the Best Cancer Hospital in Bangalore, Dasappa Cancer Hospital utilizes sophisticated clinical protocols to manage both localized and advanced disease stages. A primary component of these established protocols is radiation therapy for prostate cancer.
This therapeutic modality utilizes targeted ionizing radiation to eradicate malignant cells while preserving the functional integrity of surrounding anatomical structures.
The implementation of radiation oncology has significantly improved the clinical outcomes for patients diagnosed with prostatic adenocarcinoma. Modern radiation techniques allow for the delivery of high doses of radiation directly to the tumor site with sub-millimeter precision. This technological advancement is critical for achieving local tumor control while minimizing the dose to adjacent healthy organs, such as the bladder and the rectum.
Understanding the biophysical mechanics and the various delivery tmethods of this treatment is essential for patients and caregivers navigating the complexities of oncological care.
Medical Disclaimer
The information provided in this guide is for educational purposes only and does not constitute professional medical advice, diagnosis, or treatment. Always seek the advice of a qualified oncologist or healthcare provider with any questions regarding a medical condition. Never disregard professional medical advice or delay seeking it because of information provided in this blog.
What is radiation therapy for prostate cancer?

To fully comprehend radiation therapy for prostate cancer, patients and caregivers must examine the precise radiobiological principles that govern cellular radication. This specialized therapeutic modality does not physically extract the tumor.
Instead, it relies on the application of targeted ionizing radiation to systematically disrupt the biological replication processes of malignant prostatic tissue.
When a patient undergoes this treatment, clinical linear accelerators or precisely implanted radioactive isotopes emit high-energy photons, protons, or radioactive particles. As these emissions intersect with the targeted prostate gland, they trigger a complex biophysical reaction at the microscopic level, ultimately destroying the localized carcinoma.
The Radiobiological Process of Cellular Eradication
The destruction of malignant tissue through radiation occurs via a highly specific sequence of molecular events:
- Atomic Ionization: High-energy beams penetrate the prostatic tissue. This energy strips electrons from localized water molecules, generating highly reactive oxygen species and free radicals within the intracellular environment.
- Structural DNA Degradation: These reactive free radicals aggressively interact with the cellular DNA located inside the nucleus of the prostate cancer cells. This interaction induces severe single-strand and critical double-strand breaks within the genetic architecture.
- Replication Failure: Malignant prostate cells inherently possess defective DNA repair mechanisms when compared to adjacent healthy tissue. Consequently, they are biologically incapable of repairing these catastrophic double-strand breaks.
- Mitotic Catastrophe and Apoptosis: When the irradiated malignant cells attempt to undergo cellular division (mitosis), the severe genetic damage prevents successful replication. This structural failure triggers apoptosis, which is the programmed death of the cell, leading to gradual and sustained tumor regression over time.
In standard external beam protocols, radiation oncologists rarely deliver the total curative dose in a single administration. The standard clinical approach utilizes a schedule of fractionated doses, delivering smaller increments of radiation over multiple weeks.
This specific scheduling strategy exploits the biological differences between healthy and malignant cells. Fractionation allows adjacent healthy tissues, such as the anterior rectal wall and the bladder mucosa, sufficient time to repair sub-lethal cellular damage between treatment sessions.
Conversely, the malignant prostate cells fail to recover, accumulating the structural DNA damage until complete cellular eradication is achieved. This ensures maximum tumor control while preserving the functional integrity of the surrounding pelvic anatomy.
Types of radiation therapy for prostate cancer
The clinical selection of a specific radiation modality depends strictly on the anatomical staging of the tumor, the patient’s physiological baseline, and the precise oncological objectives established by the multidisciplinary board.
Radiation oncologists categorize these treatments into two primary delivery systems: external beam radiation and internal radioactive implantation. Understanding these distinct types of radiation therapy for prostate cancer is critical for navigating the treatment pathway.
External Beam Radiation Therapy (EBRT)
EBRT is the most frequently utilized modality for both localized and locally advanced prostate carcinoma.
This delivery system utilizes a clinical linear accelerator positioned entirely outside the patient’s body to direct high-energy photon or proton beams toward the pelvic region. Advancements in computational targeting have yielded highly sophisticated EBRT sub-categories:
- Intensity-Modulated Radiation Therapy (IMRT): IMRT utilizes advanced computer software to manipulate the intensity of individual radiation beams across the treatment field.
Conforming the radiation dose precisely to the three-dimensional shape of the prostate gland, this technique maximizes tumor eradication while significantly reducing the biological impact on the adjacent bladder and rectal tissues.
- Stereotactic Body Radiation Therapy (SBRT): SBRT delivers highly concentrated, ablative doses of radiation over a drastically reduced timeframe. It typically completes the entire treatment protocol within five individual sessions.
This modality requires supreme spatial accuracy and continuous real-time imaging to ensure the massive radiation doses are contained strictly within the prostatic volume.
- Image-Guided Radiation Therapy (IGRT): IGRT is not an independent treatment but a mandatory supportive technology utilized alongside IMRT and SBRT. It involves conducting daily imaging scans immediately before beam delivery.
This accounts for microscopic shifts in the prostate’s position caused by varying bladder and rectal volumes, ensuring absolute anatomical precision during every session.
Internal Radiation Therapy (Brachytherapy)
Brachytherapy involves the surgical placement of radioactive sources directly into the malignant prostatic tissue. This internal approach delivers a lethal, highly localized radiation dose while minimizing exposure to surrounding healthy anatomical structures.
- Low-Dose Rate (LDR) Brachytherapy: This protocol utilizes permanent radioactive seeds, typically containing Iodine-125 or Palladium-103, implanted surgically within the prostate gland. These seeds emit low levels of continuous radiation over several months, actively destroying the malignant cells before eventually decaying into inert materials.
- High-Dose Rate (HDR) Brachytherapy: HDR protocols utilize a highly radioactive source, such as Iridium-192, temporarily inserted into the prostate gland through surgical catheters. The source remains within the tissue for specific minute-long intervals to deliver a massive fractionated dose before being completely removed from the patient’s body.
Clinical Modality Comparison
To provide a clear visual overview of these protocols, the following table outlines the distinct operational parameters for each primary treatment type:
| Clinical Modality | Delivery Mechanism | Standard Treatment Duration | Primary Clinical Indication |
|---|---|---|---|
| IMRT (External) | Modulated photon beams via linear accelerator. | Daily sessions over 4 to 8 weeks. | Localized and locally advanced carcinoma. |
| SBRT (External) | Hypofractionated high-dose external beams. | 5 individual targeted sessions. | Early-stage localized carcinoma. |
| LDR Brachytherapy | Permanent surgical implantation of radioactive seeds. | Single surgical procedure; continuous emission. | Low-risk localized disease. |
| Low-risk localized disease. | Temporary catheter-based radioactive source insertion. | 1 to 3 targeted clinical sessions. | Intermediate to high-risk disease, frequently combined with EBRT. |
Meticulously matching the clinical presentation with the appropriate delivery system, oncologists can maximize the curative potential of the treatment while strictly preserving the patient’s long-term quality of life.
Side effects of radiation therapy for prostate cancer
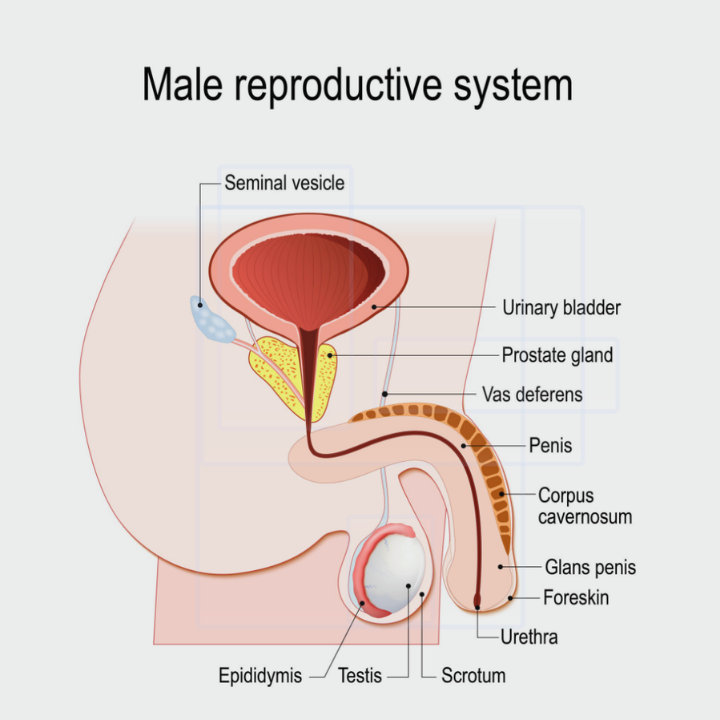
The anatomical location of the prostate gland necessitates strict precision during oncological treatment planning. As the prostate is situated immediately anterior to the rectum and inferior to the bladder, these adjacent healthy tissues inevitably absorb a fraction of the targeted radiation dose.
This localized tissue exposure is the primary biological catalyst for the side effects of radiation therapy for prostate cancer.
Radiation oncologists categorize these physiological impacts into acute and late toxicities. Acute side effects manifest during the active treatment phase or within the first 90 days following completion. These are typically driven by acute inflammatory responses and cellular DNA damage within the healthy tissue.
Conversely, late toxicities are driven by fibrotic and late immune responses, appearing months or even years after the treatment concludes. Recent clinical data establishes a definitive correlation between these phases; patients who experience moderate acute urinary or gastrointestinal toxicity are nearly twice as likely to develop severe, chronic complications.
Comprehensive Analysis of Radiation Toxicity
To provide a clear clinical expectation, the following table details the specific systemic impacts and their respective medical management protocols.
| Physiological System | Acute Manifestations (0 to 3 Months) | Chronic Manifestations (Late Toxicity) | Clinical Management Protocols |
|---|---|---|---|
| Urinary (Genitourinary) | Radiation cystitis results in frequent urination, burning sensations, and restricted urine flow. | Urethral stricture (narrowing of the urethra) and varying degrees of long-term urinary incontinence. | Pharmacological intervention with targeted alpha-blockers; potential surgical dilation for severe strictures; temporary catheterization if required. |
| Bowel (Gastrointestinal) | Radiation proctitis causes frequent bowel movements, loose stools, and acute rectal discomfort. | Chronic ulceration of the rectal wall, persistent diarrhea, and late-onset rectal bleeding. | Dietary modifications during treatment; prescription topical steroids; surgical placement of hydrogel tissue spacers before radiation. |
| Sexual and Reproductive | Temporary reduction in ejaculate volume (dry orgasm). | Progressive erectile dysfunction resulting from nerve and vascular damage; permanent infertility due to scattered radiation affecting the testicles. | Phosphodiesterase type 5 (PDE5) inhibitors for erectile support; sperm banking recommended strictly before the initiation of treatment. |
| Systemic and Dermatological | Pronounced clinical fatigue and localized skin dermatitis (reddening, peeling) at the external treatment site. | Lymphedema (fluid accumulation) in the lower extremities due to localized lymphatic node damage. | Structured resting schedules; specialized physical therapy for lymphedema management; topical application of unperfumed dermatological creams. |
Minimizing these physiological toxicities is a primary objective for the clinical team. The integration of continuous real-time imaging and the utilization of targeted radiation parameters significantly reduce the scattered dose absorbed by healthy tissues.
Patients are required to systematically report all acute symptoms to their multidisciplinary board to ensure rapid medical intervention, thereby actively mitigating the risk of long-term physiological decline.
The Workflow of Radiation Oncology
The clinical success of radiation therapy for prostate cancer depends entirely on the accuracy of the initial planning phase.
Unlike systemic treatments, radiation is a localized therapy that requires a millimeter-perfect map of the patient’s internal anatomy. At Dasappa Cancer Hospital, the workflow follows a rigorous, multi-step sequence to ensure that the maximum curative dose is delivered to the malignant tissue while strictly sparing the adjacent healthy organs.
This planning process, known as virtual simulation and dosimetry, converts diagnostic data into a precise mathematical execution plan for the linear accelerator.
Step-by-Step Clinical Workflow
- Clinical Consultation and Staging: The multidisciplinary board reviews the patient’s biopsy results, PSA levels, and Gleason score. This initial assessment determines whether the primary objective is curative or palliative.
- CT Simulation and Immobilization: The patient is placed in a customized immobilization cast to ensure identical positioning for every treatment session. High-resolution CT scans are conducted to capture the exact three-dimensional coordinates of the prostate.
- Fiducial Marker Placement: In many cases, specialized gold seeds called fiducial markers are surgically inserted into the prostate before imaging. These markers act as internal GPS points, allowing the radiation team to track the gland’s position in real time during treatment.
- Anatomical Contouring: The radiation oncologist utilizes specialized software to manually “contour” or outline the target volumes (the prostate and seminal vesicles) and the Organs at Risk (OARs), such as the rectum, bladder, and femoral heads.
- Dosimetric Planning: Medical physicists utilize sophisticated algorithms to calculate the optimal beam angles and intensities. This ensures the radiation dose conforms strictly to the target volume, a process essential for minimizing the side effects of radiation therapy for prostate cancer.
- Quality Assurance (QA) Verification: Before the first session, the plan is executed on a phantom (a specialized measuring device) to verify that the planned dose matches the actual delivery.
Target Volume Delineation Standards
To maintain absolute clinical precision, the planning team defines three distinct target volumes for every patient:
| Volume Category | Clinical Definition | Objective |
|---|---|---|
| Gross Tumor Volume (GTV) | The primary malignant mass visible on diagnostic imaging. | To ensure the core of the tumor receives the highest radiation intensity. |
| Clinical Target Volume (CTV) | The GTV plus a margin for microscopic, sub-clinical malignant extensions. | To eradicate invisible cancerous cells that may have migrated slightly beyond the visible tumor. |
| Planning Target Volume (PTV) | The CTV plus an additional margin to account for minor internal organ movement. | To ensure the tumor remains within the radiation beam despite physiological shifts in the bladder or rectum. |
Adhering to this high-density planning protocol, the clinical team can deliver various types of radiation therapy for prostate cancer with unmatched accuracy.
This systematic approach is what defines the transition from a general medical procedure to a precision-engineered oncological intervention.
Why Choose Dasappa Cancer Hospital for Radiation Oncology
Dasappa Cancer Hospital provides a specialized environment for radiation therapy for prostate cancer. The institution is led by Dr Pandu Dasappa, a senior surgical oncologist with more than 27 years of clinical experience.
- Specialized Infrastructure: The 75-bed super-specialty facility includes advanced modular operation theatres and a dedicated chemotherapy unit.
- Diagnostic Excellence: The hospital integrates comprehensive diagnostic imaging to ensure precision in treating various types of radiation therapy for prostate cancer.
- Multidisciplinary Approach: Treatment protocols are developed by a collaborative board that includes surgical, radiation, and medical oncologists.
Protocols extend beyond primary tumor eradication to include dedicated pain management, nutritional counseling, and psychosocial rehabilitation.
Conclusion
The implementation of radiation therapy for prostate cancer represents a definitive step toward local tumor control and long-term survival. By utilizing advanced delivery systems, clinicians can effectively manage prostatic malignancies while strictly minimizing the side effects of radiation therapy for prostate cancer. Dasappa Cancer Hospital remains a premier destination for Genitourinary Cancer Treatment in Bangalore, offering patients the expertise required to navigate a complex oncological journey.
As the Best Cancer Hospital in Bangalore, the hospital’s commitment is to provide precision-driven care that prioritizes both clinical efficacy and patient quality of life.