Receiving an oncological diagnosis at any phase requires immediate clinical attention, but detecting cellular abnormalities at their earliest biological stage provides the most favorable medical prognosis.
For patients seeking specialized Lung cancer treatment in Bangalore or advanced Throat cancer treatment in Bangalore, securing a comprehensive diagnostic evaluation at the Best Cancer Hospital in Bangalore is an absolute clinical priority.
When specialized oncologists diagnose a patient with stage 0 cancer, they are identifying a highly specific pathological condition where malignant cellular changes exist but have not invaded the surrounding healthy anatomical tissues.
This comprehensive medical guide details the foundational clinical concepts regarding pre-invasive malignancies. To ensure patients understand their exact physiological status, we will rigorously examine the following critical oncological areas:
- The exact microscopic pathology that strictly differentiates a non-invasive cellular dysplasia from an invasive malignant tumor.
- The specific clinical presentations and diagnostic challenges associated with identifying these localized microscopic cellular changes before systemic physiological symptoms manifest.
- The precise localized surgical and targeted intervention protocols utilized by multidisciplinary oncology teams to permanently eradicate the abnormal tissue.
Understanding the exact biological parameters of a pre-invasive diagnosis provides patients with the precise data required to make highly informed clinical decisions.
Prioritizing routine diagnostic screenings, individuals maximize their probability of intercepting cellular abnormalities before the condition requires aggressive systemic medical intervention.
What is stage 0 cancer and carcinoma in situ?
When a pathology report indicates a pre-invasive malignancy, patients immediately ask what stage 0 cancer is from a strict biological perspective. In clinical oncology, Stage 0 represents the earliest physically identifiable phase of abnormal cellular proliferation.
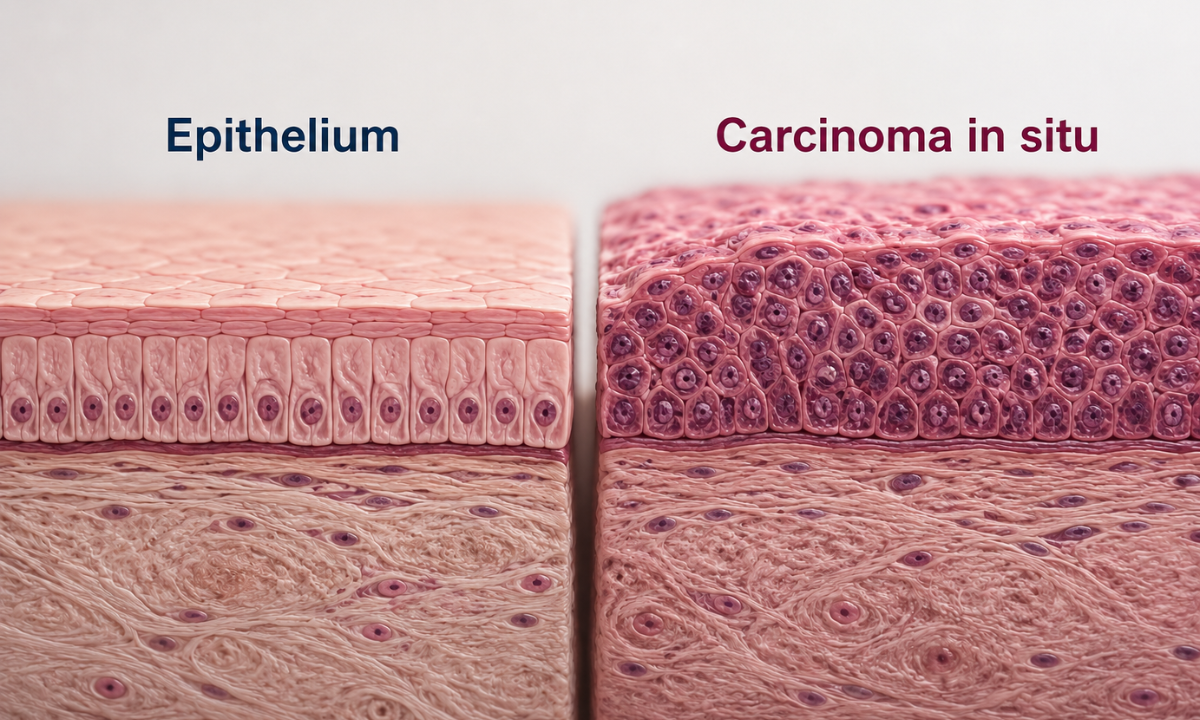
At this precise microscopic level, normal healthy cells have undergone specific genetic mutations causing them to divide erratically and form a localized cluster of malignant cells. However, this abnormal growth is strictly confined to the exact anatomical epithelial layer where it initially originated.
Medical professionals frequently utilize the diagnostic term stage 0 cancer in situ to describe this specific pathology. The Latin phrase “in situ” directly translates to “in its original place.” The critical anatomical differentiator between a Stage 0 diagnosis and an invasive malignancy is the complete structural integrity of the basement membrane.
This microscopic anatomical boundary separates the superficial surface lining of an organ from the deeper underlying connective tissues, blood vessels, and lymphatic channels.
To understand the exact clinical significance of this diagnosis, oncologists categorize cellular changes into three distinct microscopic phases.
Microscopic Pathology: The Cellular Progression Matrix
| Cellular Phase | Microscopic Characteristics | Invasion Status | Metastatic Potential |
|---|---|---|---|
| Normal Epithelium | Cells exhibit uniform size, highly organized structural arrangement, and regulated biological division. | No invasion present. | Absolute zero risk. |
| Stage 0 (Carcinoma In Situ) | Cells exhibit severe malignant mutations and disorganized division but remain strictly confined above the basement membrane. | Zero structural invasion. | Absolute zero risk. |
| Stage 1 (Invasive Carcinoma) | Malignant cells physically breach the basement membrane and infiltrate the underlying stromal tissue. | Active structural invasion. | High risk of lymphatic or vascular dissemination. |
As the malignant cells in a Stage 0 diagnosis have not breached the basement membrane, they physically cannot access the circulatory or lymphatic systems.
Therefore, biological metastasis to distant anatomical organs is an absolute physiological impossibility at this specific stage. This strict structural containment makes the condition highly curable. However, if the medical team does not surgically excise or ablate these abnormal cells, the continuous genetic mutations will inevitably grant the cells the biological capability to destroy the basement membrane, forcing the diagnosis to progress into an invasive and potentially fatal carcinoma.
Diagnosing stage 0 cancer symptoms
The primary clinical challenge associated with pre-invasive malignancies is the profound lack of physical warning signs. When patients inquire about typical stage 0 cancer symptoms, oncologists must clarify that this specific biological phase is predominantly asymptomatic. This absence of symptoms is a direct result of the strict microscopic localization of the abnormal cells.
Because Stage 0 carcinoma in situ is physically restricted to the superficial epithelial layer, the malignant cells have not penetrated the basement membrane.
Consequently, these cells do not interact with the underlying vascular networks, lymphatic channels, or neurological infrastructures. Without this structural interaction, the biological triggers that typically produce pain, localized bleeding, or systemic inflammation remain completely unactivated.
The patient’s immune system frequently does not mount a massive systemic response, allowing the microscopic dysplasia to remain entirely undetected by the host. Patients diagnosed with Stage 0 disease will rarely experience the systemic physiological indicators associated with advanced oncology.
Absent Systemic Indicators in Pre-Invasive Disease
- No Unexplained Weight Loss: The localized cellular growth does not generate the massive metabolic demand required to cause sudden physiological wasting.
- No Chronic Fatigue: The absence of systemic inflammation prevents the profound biological exhaustion typically associated with invasive tumors.
- No Systemic Pain: The abnormal cells do not physically compress underlying nerve endings or infiltrate surrounding organ capsules.
- No Spontaneous Hemorrhage: The cells have not degraded the structural integrity of the underlying blood vessels, preventing the internal bleeding common in later stages.
Due to this completely asymptomatic presentation, physical symptom manifestation is a highly unreliable metric for early detection of cancer. If a patient waits for definitive physiological pain or dysfunction to appear, the biological reality is that the malignancy has already progressed significantly beyond Stage 0.
Therefore, the clinical identification of pre-invasive cellular dysplasia relies almost exclusively on proactive diagnostic imaging and routine pathological screening.
The vast majority of Stage 0 diagnoses are secured through preventative procedures such as routine colonoscopies, mammograms, Papanicolaou (Pap) smears, or low-dose computed tomography scans for high-risk demographic groups.
These specialized diagnostic protocols are explicitly designed to visualize or extract microscopic cellular abnormalities long before they possess the biological capability to generate physical symptoms.
Respiratory and Otolaryngological Signs

While systemic physiological responses are definitively absent during pre-invasive malignancy, highly localized cellular dysplasia can occasionally generate microscopic physical disruptions. These disruptions occur exclusively when the abnormal cellular growth develops in anatomical regions subjecte
d to constant physiological friction, continuous airflow, or active mechanical vibration.
Consequently, patients and medical professionals must remain highly vigilant regarding specific micro-symptoms, particularly within the respiratory and head and neck systems.
Evaluating Respiratory Indicators
The human pulmonary system presents a severe diagnostic challenge because the deep lung parenchyma completely lacks internal pain receptors.
Therefore, microscopic dysplasia developing in the outer periphery of the lungs will remain entirely silent. However, when abnormal cells develop centrally within the major bronchial airways, the localized irritation can trigger subtle physiological responses.
When clinical pulmonologists evaluate potential stage 0 lung cancer symptoms, they specifically monitor for the following localized airway disruptions:
- Atypical Chronic Cough: A persistent cough that does not resolve with standard antibiotic or antitussive medications. This occurs as the bronchial mucosa attempts to clear the localized cellular irregularity.
- Trace Hemoptysis: The observation of microscopic amounts of blood within the sputum. This is caused by the superficial ulceration of the fragile pre-invasive cells during the mechanical stress of a forced cough.
- Localized Wheezing: A subtle, high-pitched respiratory sound isolated to a single specific airway. This indicates a minor aerodynamic disruption caused by the microscopic cellular cluster restricting localized airflow.
Patients frequently misattribute these subtle respiratory indicators to benign environmental allergies or chronic bronchitis, delaying necessary diagnostic imaging.
Evaluating Otolaryngological Indicators
The mucosal linings of the pharynx and the delicate muscular structures of the larynx are highly sensitive to microscopic structural changes. Because the vocal cords require absolute symmetrical precision to produce clear phonation, even a microscopic cluster of abnormal surface cells will disrupt acoustic resonance.
When specialized otolaryngologists assess stage 0 throat cancer symptoms, they look for specific mucosal and mechanical alterations during endoscopic visualization:
- Dysphonia: Persistent hoarseness or a fundamental change in vocal pitch lasting longer than three weeks. This is the primary mechanical indicator of cellular dysplasia forming directly on the vocal folds.
- Visual Mucosal Dysplasia: The clinical observation of leukoplakia (thickened white patches) or erythroplakia (abnormal red vascular patches) on the mucosal surface. These lesions represent areas of rapid, disorganized cellular turnover.
- Localized Odynophagia: A highly specific, unilateral pain when swallowing that remains localized to one exact anatomical point in the throat, indicating localized mucosal inflammation.
Recognizing these site-specific diagnostic signs is absolutely critical. Identifying these micro-symptoms prompts the immediate utilization of specialized endoscopic evaluations or targeted tissue biopsies, allowing the clinical oncology team to confirm the pre-invasive diagnosis before the basement membrane is breached.
Stage 0 Cancer Treatment Protocols

The primary oncological objective for managing pre-invasive cellular dysplasia is the complete physical eradication of the abnormal tissue while strictly preserving the surrounding healthy anatomical structures.
As Stage 0 carcinoma in situ lacks the biological capability to metastasise, systemic interventions such as intravenous chemotherapy or broad-field radiation are clinically unnecessary and generally contraindicated. Instead, multidisciplinary oncology teams utilize highly targeted, localized stage 0 cancer treatment protocols.
The specific interventional modality selected depends entirely on the anatomical location of the dysplasia and the total surface area of the microscopic cellular cluster. Clinical specialists divide these localized treatments into two primary categories: surgical excisions and targeted ablations.
Targeted Surgical Excision Modalities
Surgical excision involves the precise physical removal of the abnormal cellular tissue along with a microscopic margin of healthy tissue. This guarantees complete eradication and provides an intact tissue sample for final pathological verification.
| Excision Technique | Clinical Application | Procedural Mechanism |
|---|---|---|
| Endoscopic Mucosal Resection (EMR) | Gastrointestinal or respiratory surface dysplasia. | Utilizes a specialized endoscope to inject fluid beneath the lesion, lifting the abnormal mucosa before excising it with a specialized wire loop. |
| Wide Local Excision | Superficial dermal or mammary tissue abnormalities. | Surgically removes the primary cellular cluster along with a strictly measured perimeter of surrounding healthy cells to ensure absolute margin clearance. |
| Loop Electrosurgical Excision | Cervical or localized mucosal carcinoma in situ. | Deploys a thin, low-voltage electrified wire loop to precisely cut away the abnormal epithelial layer while simultaneously coagulating local blood vessels. |
Advanced Ablative Interventions
When surgical excision is anatomically challenging or poses a risk to delicate surrounding structures, oncologists utilize ablative therapies. These protocols physically destroy the abnormal cells in their exact location without removing a physical tissue sample.
- Cryoablation Therapy: The clinical application of extreme, localized cold utilizing liquid nitrogen or argon gas. This rapidly freezes the intracellular fluid of the abnormal cells, causing immediate cellular death and subsequent tissue sloughing.
- Radiofrequency Ablation (RFA): The insertion of a highly specialized probe directly into the dysplastic cluster. The probe emits high-frequency electrical currents that generate intense localized heat, thermally coagulating and destroying the pre-invasive cells.
- Photodynamic Therapy (PDT): The administration of a photosensitizing pharmacological agent that accumulates specifically within the rapidly dividing abnormal cells. The clinical team then applies a specific wavelength of laser light to the area, triggering a localized chemical reaction that destroys the targeted cells.
- Laser Vaporization: The utilization of highly concentrated, high-intensity beams of light to precisely heat and vaporize the superficial layer of abnormal cells, leaving the underlying basement membrane and connective tissue completely intact.
Post-Intervention Clinical Objectives
Following the successful execution of any stage 0 cancer treatment, the patient transitions into a rigorous observation phase. The clinical team monitors the patient to ensure several critical oncological objectives have been achieved:
- Histological Margin Confirmation: For excisional procedures, pathologists must verify that the outer edges of the removed tissue are completely free of any malignant mutations.
- Organ Function Preservation: Ensuring that the localized treatment did not structurally compromise the physiological function of the underlying organ system.
- Recurrence Surveillance: Establishing a strict schedule for routine localized endoscopic or radiological screenings to immediately identify any new cellular abnormalities that may develop in the adjacent epithelial tissues.
Utilizing these highly precise localized protocols, oncologists permanently neutralize the threat of cellular invasion, providing patients with a definitive clinical resolution while allowing them to maintain an optimal baseline of physiological function.
Why Choose Dasappa Cancer Hospital
Selecting an oncology facility for the management of pre-invasive cellular dysplasia requires a strict commitment to diagnostic accuracy and tissue-preserving surgical precision. Dasappa Cancer Hospital provides a premier clinical environment specifically engineered to intercept and eradicate malignancies at their absolute earliest biological stages.
Our multidisciplinary oncology boards operate strictly under international evidence-based guidelines, ensuring that every patient receives a highly customized, localized treatment protocol.
Several definitive clinical factors distinguish Dasappa Cancer Hospital as a leading institution for early-stage oncological intervention:
- High-Resolution Diagnostic Imaging: Our facility is equipped with advanced low-dose computed tomography and high-definition endoscopic technology, enabling our clinical team to visualize microscopic mucosal and epithelial irregularities long before they become invasive.
- Specialized Surgical Oncology: Our surgical departments specialize in minimally invasive and organ-preserving excision techniques, including advanced endoscopic mucosal resections and precise laser ablations.
- Expert Histopathological Analysis: We maintain an elite in-house pathology laboratory that provides rapid, highly accurate cellular evaluations to guarantee absolute margin clearance following any localized surgical intervention.
- Comprehensive Surveillance Programs: We establish rigorous post-treatment monitoring protocols to ensure long-term clinical stability and immediately identify any potential cellular recurrences.
As you choose Dasappa Cancer Hospital, we guarantee that the patient’s pre-invasive diagnosis is managed utilizing the most advanced localized interventional technology available, completely prioritizing both permanent oncological eradication and the preservation of long-term physiological function.
Conclusion
A diagnosis of Stage 0 carcinoma in situ represents a highly favorable clinical scenario where the abnormal cellular growth is completely isolated and entirely curable. Because these microscopic cellular changes rarely produce systemic physical symptoms, relying on physiological warning signs is a dangerous and highly flawed diagnostic strategy. The biological reality dictates that waiting for pain or dysfunction strictly allows the malignancy the time required to breach the basement membrane and become an invasive threat.
Do not allow microscopic cellular dysplasia the opportunity to progress into systemic disease. Prioritize your long-term physiological stability by adhering to routine preventative screening schedules. Contact the specialized oncology coordination team at Dasappa Cancer Hospital today to schedule your comprehensive diagnostic evaluation, secure your clinical baseline, and ensure any localized abnormalities are permanently eradicated at their earliest biological stage.