For individuals confronting advanced abdominal malignancies that have seeded across the delicate peritoneal lining, conventional systemic options often present a biological dead end. The development of intraoperative hipec surgery has drastically redefined the paradigm of surface malignancy care by shifting from systemic drug circulation to targeted, localized hyperthermic destruction.
Evaluating clinical candidacy at the Best cancer hospital in Bangalore provides families with the advanced multi disciplinary expertise required to transform an intimidating diagnosis into a highly structured, precision driven surgical strategy. Addressing advanced disease at its direct anatomical site, this unique approach opens an aggressive avenue for long term survivorship.
To appreciate the medical reasoning behind this approach, it helps to look at the unique way certain abdominal tumors grow. Primary malignancies originating in the appendix, ovaries, colon, or stomach frequently shed malignant cells directly into the peritoneal cavity.
These cells drift through the natural lubricating fluid of the abdomen, eventually anchoring to the peritoneum the expansive membrane that covers and protects your digestive organs. Once established, these micro deposits form a widespread web of surface tumors.
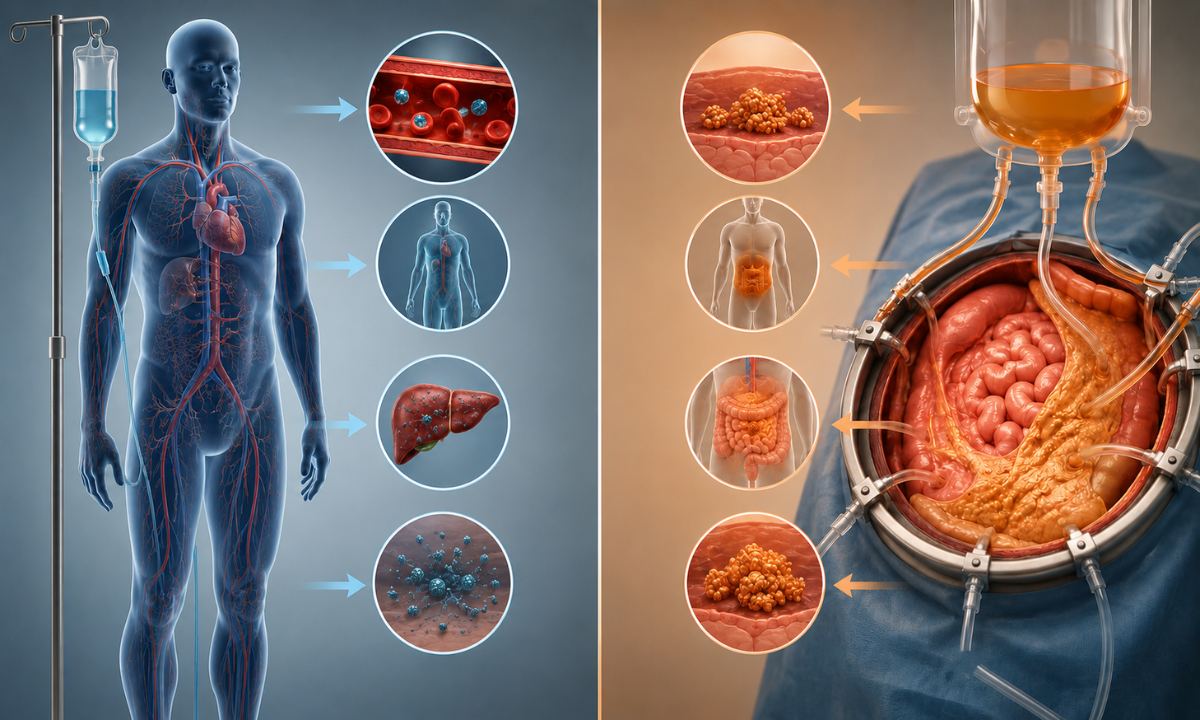
Traditional cancer therapies struggle significantly with surface spread because of a tough physical wall known as the peritoneal plasma barrier. This anatomical shield, made up of tight cell junctions and blood vessel walls, limits standard intravenous (IV) chemotherapy from crossing over into the abdominal cavity fluid in meaningful amounts.
To get enough medication past this barrier using an IV, a doctor would have to prescribe doses so high they would cause dangerous, toxic side effects throughout the entire body.
Intraoperative hyperthermic perfusion elegantly bypasses this biological limitation. Instead of relying on the bloodstream to carry medications, the surgical team delivers a highly concentrated, pre warmed chemotherapeutic solution straight into the open abdomen. This direct delivery allows the medicine to stay contained within the abdominal cavity, safely shielded by the very barrier that once blocked standard treatment. As a result, the rest of the body is protected from severe systemic side effects, allowing oncology teams to safely maximize the dose directly at the root of the disease.
Medical Disclaimer
The surgical overviews, biological concepts, and recovery guidelines detailed throughout this article are intended solely for public health awareness and educational purposes. This informational material does not function as a replacement for expert medical advice, direct clinical diagnoses, official therapeutic prescriptions, or individualized healthcare strategies. Peritoneal surface malignancies are exceptionally complex and require highly individualized diagnostic staging and multi disciplinary evaluation. Always consult a qualified surgical oncologist, medical oncologist, or board certified physician to thoroughly review your unique medical condition or specific treatment parameters. Never disregard, avoid, or delay professional medical consultations because of the educational concepts discussed in this document.
The First Step is the Maximal Tumor Clearance
Before the heated chemotherapeutic fluid can ever be introduced into the abdominal cavity, the surgical team must execute the most physically demanding phase of the procedure. This foundational stage, known clinically as cytoreduction surgery, focuses on the meticulous, manual removal of every single visible tumor nodule, affected organ tissue, or surface mass within the abdomen. The ultimate success of the subsequent heated liquid wash relies entirely on the thoroughness of this physical debulking phase.
Why must surgical extraction precede the chemical wash? The heated chemotherapeutic solution delivered afterward has a finite microscopic penetration depth, typically reaching only 2 to 3 millimeters into remaining tissue surfaces. If macro sized tumor masses anything larger than the size of a small pebble are left behind, the fluid wash will merely coat the exterior of the mass, leaving the deep cancer cells inside completely untouched.
During this meticulous macroscopic clearance phase, the surgical oncology team systematically evaluates the 13 distinct regions of the abdominal cavity, mapping out the disease spread to perform a series of complex resections:
- Peritonectomy: Stripping away sections of the diseased peritoneal lining where tumor cells have anchored and spread.
- Omentectomy: Removing the omentum the large fatty apron covering the intestines which frequently acts as a primary landing zone for floating cancer seeds.
- Targeted Organ Resections: Safely removing involved organs or parts of organs, such as the appendix, gallbladder, spleen, or specific segments of the small and large intestines, depending on the extent of localized tumor invasion.
The overarching goal of this aggressive surgical phase is to achieve what is called an “optimal cytoreduction,” meaning no visible tumor larger than 2.5 millimeters remains behind.
Clearing away these physical macro blockades, the surgical team transforms a complex, bulky disease state into a microscopic target field, setting the stage for the heated chemical wash to deliver its maximum molecular impact.
Bypassing the Peritoneal Shield and The Molecular Fluid Wash
Once the macroscopic debulking phase is complete, the surgical team transitions to the microscopic eradication phase. Combining standard mechanical cytoreduction with hipec surgery creates a dual action therapeutic strategy designed to eliminate the remaining invisible cancer cells floating inside the abdominal cavity. By shifting the delivery mechanism from the general bloodstream to a localized liquid wash, this technique safely exposes hidden micro metastases to high concentration medications that would otherwise be unsafe to administer systemically.
The Biophysics of Thermal Synergy
The true power of this chemical wash relies on warming the chemotherapeutic solution precisely between 41°C and 43°C. This hyperthermic state acts as a powerful multiplier for the medication through distinct biological mechanisms:
- Increased Cell Wall Permeability: The localized heat physically distorts the outer lipid membrane of cancer cells, making them more porous and allowing the chemotherapy drugs to enter the cell interior much more rapidly.
- Enhanced Tissue Penetration: At normal body temperature, liquid chemotherapy only skims the outermost layers of tissue. Elevating the temperature allows the fluid to penetrate between 2 and 3 millimeters deep into the remaining tissue beds, reaching cells hidden beneath the surface.
- Selective Cytotoxicity: Malignant cells possess primitive, disorganized blood vessel networks that cannot dissipate heat efficiently. While normal tissues can handle a temporary temperature increase, the cancer cells overheat, damaging their internal DNA repair mechanisms and accelerating cell death.
- Altered Cellular Microenvironment: The heat induces mild oxidative stress within the remaining tumor beds, actively blocking the cancer cells’ ability to recover from the chemical damage delivered by the medicine.
Pharmacokinetic Advantages: Intravenous vs. Intraperitoneal Delivery
To understand why this approach is highly effective for peritoneal surface diseases, it is valuable to evaluate how it compares directly with traditional systemic treatments:
| Therapeutic Parameter | Standard Intravenous (IV) Chemotherapy | Hyperthermic Intraperitoneal Chemotherapy (HIPEC) |
|---|---|---|
| Primary Delivery Route | Circulated globally through the main bloodstream | Perfused directly inside the open abdominal cavity |
| Anatomical Barriers Encountered | Must cross the highly restrictive peritoneal plasma barrier | Completely bypasses the peritoneal shield through direct contact |
| Localized Drug Concentration | Low to moderate at the actual tumor surface | Exceptionally high (up to 20 times the systemic dose) |
| Systemic Toxicity Profile | High risk of widespread side effects (hair loss, severe nausea, bone marrow suppression) | Minimal systemic exposure as the drugs remain trapped inside the abdomen |
| Primary Target Domain | Macro metastases with rich, active internal blood supplies | Microscopic tumor residue and floating cancer cells post debulking |
By using these advanced fluid mechanics, the oncology team turns the abdomen’s natural defensive lining into an asset, trapping the high concentration medication exactly where it is needed most to sterilize the abdominal environment.
Inside the Operating Theater: Timing and Workflow
A combined intraperitoneal procedure is one of the most sophisticated and highly coordinated operations performed in modern surgical oncology. The operating theater transforms into a dual specialty environment where the surgical team works in tandem with advanced perfusion technologists and specialized oncology anesthesiologists. Understanding the exact mechanical timeline inside the room helps demystify the complexity of this comprehensive intervention for patients and their families.
The Two-Phase Intraoperative Roadmap
- The Surgical Resection Phase: This initial period consumes the largest portion of the operational window. The surgical team carefully explores the abdominal cavity, identifying all visible surface deposits and performing necessary organ resections to clear the macro disease. Because every millimeter of tissue must be inspected, this manual debulking requires extreme patience, precision, and surgical stamina.
- The Chemotherapeutic Perfusion Phase: Once the abdomen is cleared of visible disease, the perfusion team steps in. Specialized inflow and outflow catheters are placed directly into the abdominal cavity and connected to a dedicated hyperthermic perfusion machine. This external circuit continuously warms, filters, and pumps the high concentration medication throughout the abdomen, maintaining a strict temperature matrix for a set period (typically 60 to 90 minutes) before the fluid is completely drained.
Understanding the Total Time Investment
Because this dual stage process combines extensive structural tissue removal with advanced molecular fluid dynamics, the total hipec surgery duration can be highly variable, frequently spanning anywhere from 6 to 14 hours. The precise time required depends entirely on the volume of tumor seeding encountered during the initial exploration, the number of abdominal organs requiring resection, and the complexity of reconstructing the digestive tract after the tissues are cleared.
The Anesthetic and Metabolic Balancing Act

- Core Temperature Regulation: While the abdominal cavity is intentionally heated to 42°C, the rest of the patient’s body must maintain normal baseline temperatures. Anesthesiologists utilize advanced cooling blankets and chilled intravenous fluids to protect the brain and upper organs from systemic overheating.
- Hemodynamic and Fluid Management: The combination of extensive tissue removal and heated fluid perfusion can cause rapid fluid shifts within the body. Continuous arterial monitoring ensures that blood pressure remains perfectly stable throughout the entire wash.
- Renal Protection Protocols: High dose abdominal chemotherapy puts temporary strain on the kidneys as the body begins to clear the medication. The medical team maintains high intravenous fluid volumes and monitors urine output minute by minute to shield kidney function from stress.
By coordinating these intricate physical and chemical systems in real time, the operating team ensures that the entire procedure moves forward with maximum safety, laying a secure foundation for the patient’s subsequent healing phase.
Why Choose Dasappa Cancer Hospital for Complex Care?
Recovering from an extensive abdominal intervention requires a specialized postoperative care network. At Dasappa Cancer Hospital, understanding what to expect after HIPEC surgery helps patients and their caregivers navigate the healing process with realistic expectations. Immediately following the operation, patients are transitioned to our specialized Surgical Intensive Care Unit (SICU) for close monitoring. The combination of extensive tissue removal and heated perfusion temporarily disrupts normal digestive function, resulting in a temporary paralysis of the bowel (ileus). To manage this safely, our multidisciplinary team utilizes central venous lines to deliver Total Parenteral Nutrition (TPN), ensuring the body receives essential nutrients, fluids, and electrolytes while the gastrointestinal tract rests and heals during the initial recovery period.
Our advanced treatment framework provides patients with dedicated institutional advantages:
- Expert Surgical Leadership: Guided by Dr. Pandu Dasappa, a veteran Senior Surgical Oncologist with over 27 years of experience in complex abdominal resections and advanced cytoreductive procedures.
- Dedicated 75 Bed Specialized Infrastructure: Located in Basavanagudi, our super specialty facility features modular operating theaters and dedicated critical care units customized specifically for oncology patients.
- Comprehensive Nutritional Rehabilitation: A personalized dietary team oversees advanced metabolic support, managing central lines and specialized liquid nutrition to optimize healing.
- Integrated Pain and Supportive Management: Continuous pain control protocols are customized to ensure patient comfort, promoting early movement and preventing chest complications.
The average cytoreductive surgery recovery time spent inside the hospital typically spans 10 to 14 days, depending on how quickly normal bowel function returns and general physical mobility is achieved. Our step by step rehabilitation protocol is designed to transition patients safely from absolute rest to independent daily living, providing families with continuous guidance at every stage of the recovery journey.
Conclusion
Facing an advanced peritoneal malignancy requires a treatment plan that balances aggressive medical engineering with a compassionate, patient first approach. By combining physical tumor removal with high concentration thermal perfusion, this multi stage operation offers a powerful alternative for tumors that once had limited options. Choosing an experienced, dedicated team gives families the clinical precision and comprehensive support needed to face complex cancer treatments with true resilience and absolute confidence.