Patients diagnosed with severe hematological malignancies, such as leukemia, lymphoma, or multiple myeloma, require immediate and aggressive medical intervention.
Seeking treatment at a premier Cancer Hospital in Bangalore ensures access to the highly specialized clinical infrastructure necessary for managing these complex systemic diseases. As the Best Cancer Hospital in Bangalore, Dasappa Cancer Hospital provides advanced curative protocols for patients facing these aggressive conditions.
One of the most intensive and potentially curative procedures utilized by our oncology team is the replacement of damaged hematopoietic stem cells. Understanding the specific types of bone marrow transplantation is a critical first step for patients preparing to undergo this rigorous clinical pathway.
A bone marrow transplant, formally classified as a hematopoietic stem cell transplant, is not a surgical operation. It is a highly controlled, intravenous medical infusion of healthy stem cells.
This procedure is designed to completely rescue and rebuild the patient’s blood forming system after it has been intentionally eradicated by high doses of chemotherapy or targeted radiation. Because this intensive intervention carries significant clinical risks and requires meticulous biological matching, this comprehensive guide will detail the exact protocols involved.
We will systematically explore the clinical nuances of this advanced hematological procedure by addressing the following critical areas:
- The biological mechanism of stem cell rescue: We will explain exactly why high dose oncology treatments necessitate the subsequent total replacement of the patient’s marrow.
- The distinct procedural modalities: We will detail the exact medical differences between utilizing a patient’s own previously harvested cells versus sourcing healthy cells from a genetically matched donor.
- Patient eligibility and outcome statistics: We will outline the strict medical criteria required for qualification and provide an objective review of long term survival and disease remission rates.
- The logistical and financial considerations: We will address the practical aspects of undergoing this extensive, multi phase treatment within a specialized tertiary care facility.
Thoroughly understanding these specific clinical parameters, patients and their families can make highly informed, evidence based decisions regarding their long term hematological care.
The Clinical Necessity of Stem Cell Replacement

To understand the exact medical justification for a bone marrow transplant, patients must first understand the fundamental biological function of the human hematopoietic system.
Bone marrow is the soft, spongy tissue located within the central cavities of specific large bones, primarily the pelvis, sternum, and femurs. This specialized tissue serves as the biological source for the entire circulatory and immune systems.
It houses immature, unspecialized cells known as hematopoietic stem cells. Through a continuous biological process called hematopoiesis, these specific stem cells divide and mature into three vital blood components:
- Erythrocytes (Red Blood Cells): Responsible for transporting oxygen from the lungs to the systemic cellular tissues.
- Leukocytes (White Blood Cells): The primary cellular components of the immune system, responsible for identifying and destroying infectious pathogens.
- Thrombocytes (Platelets): Cell fragments that strictly regulate hemostasis by initiating blood clotting and preventing uncontrolled hemorrhage.
In severe hematological malignancies such as leukemia, lymphoma, and multiple myeloma, the cellular mutation originates directly within these stem cells or their immediate lineage.
The malignant cells rapidly multiply, physically overcrowding the marrow cavity and aggressively suppressing the production of healthy blood components.
To achieve permanent disease remission, oncologists must administer exceptionally high doses of systemic chemotherapy, often combined with total body irradiation. The primary medical objective of these aggressive treatments is to completely eradicate every malignant cell within the body.
However, these powerful pharmacological and radiological interventions are not completely selective. As they destroy the cancer, they simultaneously cause severe myeloablation, meaning they permanently destroy the patient’s healthy hematopoietic stem cells in the process.
Following this massive oncological intervention, the patient is left without a functioning immune system and without the biological capacity to produce new blood cells naturally.
Therefore, the bone marrow transplant is not actually the direct treatment for the cancer itself. The high dose chemotherapy and radiation constitute the cancer treatment. The transplant is a mandatory clinical rescue procedure. By intravenously infusing healthy hematopoietic stem cells into the patient’s bloodstream immediately following the intensive therapy, the medical team provides the exact biological material required.
These infused cells naturally migrate into the empty bone cavities, engraft within the tissue, and completely regenerate a healthy, fully functional hematopoietic and immune system.
Utilizing the Patient’s Cells
Among the primary types of bone marrow transplantation, the autologous protocol relies entirely on the patient’s own biological material.
This specific procedure is highly effective for treating malignancies that typically do not directly involve heavy contamination of the bone marrow cavity, such as multiple myeloma, Hodgkin lymphoma, and specific variations of Non Hodgkin lymphoma.
Utilizing the patient’s own hematopoietic stem cells, the clinical team completely eliminates the severe risk of immunological rejection, making it a safer alternative when medically appropriate.
The autologous transplant is not a single event but rather a carefully orchestrated, multi phase clinical process. The oncology team must safely extract the healthy cells before administering the toxic, high dose cancer treatments.
The Sequential Phases of an Autologous Transplant
Mobilization and Collection
The patient receives targeted daily subcutaneous injections of specific growth factors, such as Granulocyte Colony Stimulating Factor.
These medications force the bone marrow to rapidly produce and release immature stem cells directly into the peripheral bloodstream. The medical team then extracts these specific cells utilizing an intravenous apheresis machine, which filters the stem cells and immediately returns the remaining blood components to the patient.
Cellular Cryopreservation
The harvested stem cells are meticulously processed in a highly controlled clinical laboratory.
Technicians mix the cells with a specialized chemical preservative solution and freeze them at extreme subzero temperatures to maintain absolute cellular viability during the patient’s upcoming cancer treatment.
Myeloablative Conditioning
The patient is admitted to the oncology ward and receives intensive, high dose chemotherapy or targeted radiation therapy.
This aggressive regimen is specifically designed to eradicate the existing malignant cells circulating within the body, simultaneously destroying the remaining bone marrow in the process.
Stem Cell Reinfusion
Following the completion of the intensive conditioning regimen and a mandatory rest period to allow the toxic chemotherapy drugs to clear the system, the frozen stem cells are carefully thawed.
The medical team intravenously infused these cells back into the patient’s central venous catheter.
Hematopoietic Engraftment
The newly infused stem cells naturally migrate through the bloodstream, locate the empty bone marrow cavities, and permanently engraft.
Within two to four weeks, these cells begin synthesizing a completely new supply of healthy red blood cells, white blood cells, and platelets.
To evaluate whether this specific procedural modality is appropriate, the multidisciplinary oncology board reviews the patient’s exact diagnosis and physiological status.
Clinical Profile of Autologous Transplantation
| Clinical Parameter | Autologous Transplant Characteristics |
| Primary Indications | Multiple Myeloma, Relapsed Hodgkin Lymphoma, Relapsed Non Hodgkin Lymphoma, Neuroblastoma. |
| Immunological Rejection Risk | Statistically zero, as the biological material belongs entirely to the patient. |
| Graft Versus Host Disease (GVHD) | Impossible, due to the exact genetic match of the infused hematopoietic cells. |
| Graft Versus Tumor Effect | Absent. The procedure relies entirely on the conditioning chemotherapy to completely eradicate the malignancy. |
| Tumor Cell Contamination Risk | Present. There is a minor clinical risk that microscopic cancer cells may be inadvertently harvested and reinfused alongside the healthy stem cells. |
Safely storing the patient’s own healthy stem cells prior to the administration of lethal doses of chemotherapy, oncologists can aggressively treat the underlying malignancy while guaranteeing a successful hematopoietic rescue.
Sourcing from a Matched Donor
The second primary classification is the allogeneic bone marrow transplant. This intensive protocol utilizes hematopoietic stem cells harvested from a healthy, genetically matched donor rather than the patient.
Oncologists mandate this specific modality for aggressive malignancies that heavily infiltrate the bone marrow cavity, such as Acute Lymphoblastic Leukemia, Acute Myeloid Leukemia, and severe myelodysplastic syndromes.
In these specific clinical scenarios, the patient’s native stem cells are typically too genetically corrupted or physically depleted to be safely reinfused.
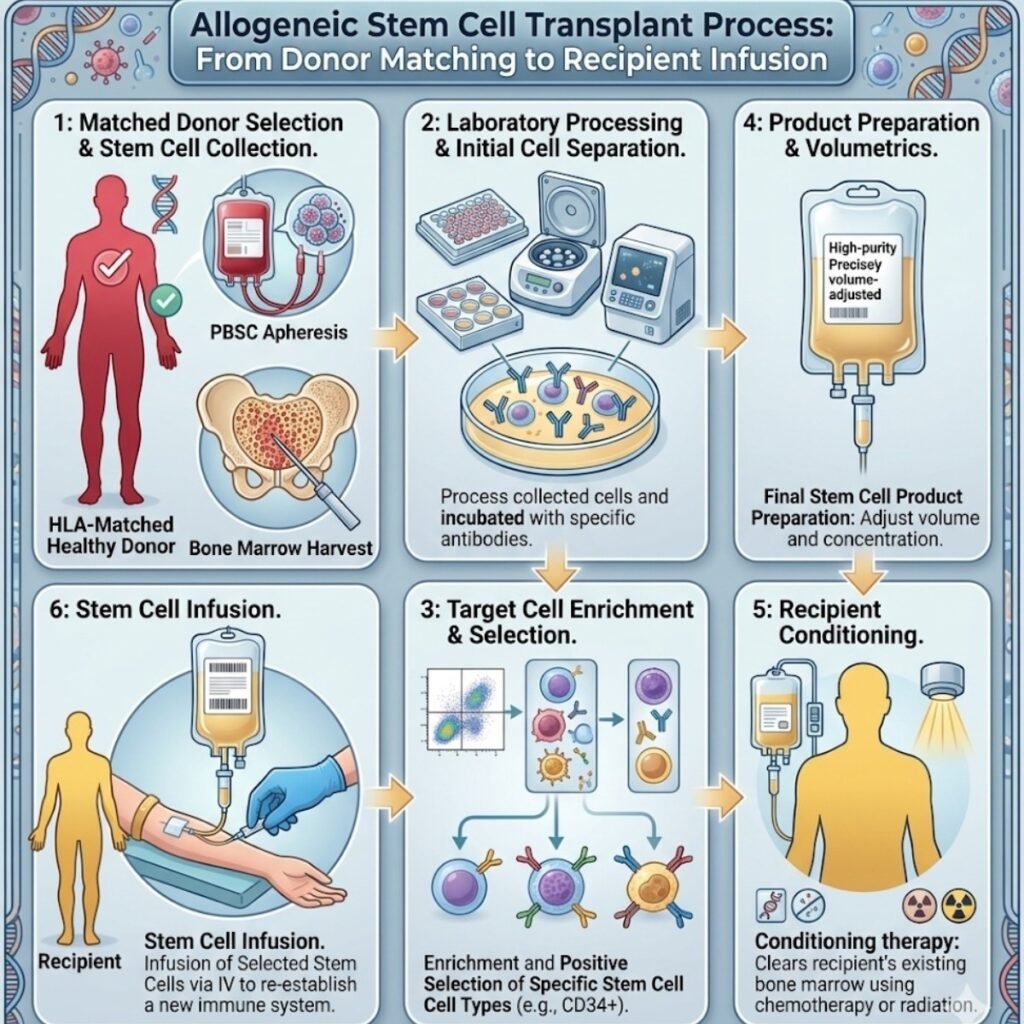
The defining complexity of an allogeneic transplant is the absolute requirement for precise immunological compatibility. To prevent immediate biological rejection, the clinical team must carefully evaluate and select a donor based on strict genetic criteria.
The Clinical Sequence of Allogeneic Transplantation
Human Leukocyte Antigen Typing
The medical team conducts specialized blood testing to map the specific Human Leukocyte Antigen markers present on the surface of the patient’s cells.
These inherited genetic proteins strictly dictate how the immune system distinguishes native biological tissues from foreign cellular material.
Donor Identification
The optimal biological source is typically a fully matched sibling. If a familial match is clinically unavailable, the oncology team will search global stem cell registries to locate a matched unrelated donor.
Modern hematological advancements also permit the use of haploidentical donors, which are half matched family members, or the utilization of thoroughly screened umbilical cord blood.
Immunosuppressive Conditioning
Prior to the cellular infusion, the patient undergoes aggressive myeloablative chemotherapy paired with highly potent immunosuppressive medications.
This critical regimen serves a dual purpose: it eradicates the circulating malignancy and intentionally disables the patient’s existing immune system to prevent it from attacking the incoming donor cells.
Donor Cell Engraftment
Following the intravenous infusion, the foreign stem cells migrate into the patient’s bone marrow cavities.
Over the subsequent weeks, these donor cells begin synthesizing a completely new immune system utilizing the donor’s exact genetic blueprint.
Because the allogeneic protocol introduces an entirely new, active immune system into the patient’s body, it creates two unique and opposing biological phenomena that the oncology team must continuously monitor and manage.
Immunological Dynamics of Allogeneic Transplantation
| Clinical Phenomenon | Physiological Mechanism | Clinical Impact |
| Graft Versus Host Disease (GVHD) | The newly established donor immune cells fail to recognize the patient’s native organs as safe tissue and systematically attack the patient’s skin, liver, or gastrointestinal tract. | Represents a severe, potentially life threatening systemic complication that strictly requires long term management with specialized immunosuppressive pharmacological therapies. |
| Graft Versus Tumor Effect (GVT) | The newly established donor immune cells actively recognize, target, and destroy any microscopic malignant cells that successfully survived the initial high dose chemotherapy conditioning. | Represents a highly beneficial, curative immunological response that drastically reduces the statistical probability of a future cancer relapse. |
Meticulously balancing the potent immunological power of the donor cells against the severe risks of tissue rejection, the hematology team leverages the allogeneic transplant to effectively eradicate aggressive, treatment resistant blood cancers.
Patient Eligibility and Clinical Criteria
Because a bone marrow transplant imposes extreme physiological stress on the human body, not every patient diagnosed with a qualifying hematological malignancy is a medically appropriate candidate.
Prior to clinical approval, the multidisciplinary oncology board mandates a comprehensive physiological evaluation to ensure the patient possesses the physical resilience required to survive the myeloablative conditioning and the subsequent period of profound immunosuppression.
Comprehensive Pre Transplant Physiological Evaluation
The clinical team conducts a systematic review of all major organ systems. The high dose chemotherapy utilized in the conditioning phase possesses severe systemic toxicity. Therefore, the patient must demonstrate optimal baseline organ function before the procedure can safely commence.
- Cardiovascular Assessment: An echocardiogram and an electrocardiogram are strictly required to evaluate the mechanical pumping efficiency and the electrical stability of the heart muscle.
- Pulmonary Function Testing: Detailed spirometry tests measure total lung capacity and the efficiency of oxygen exchange, ensuring the respiratory system can withstand potential infectious complications during the deeply immunocompromised phase.
- Hepatic and Renal Panels: Comprehensive metabolic blood tests quantify liver enzymes and kidney filtration rates. These organs are primarily responsible for metabolizing and excreting the massive doses of chemotherapy drugs, making their optimal function a strict prerequisite.
- Infectious Disease Screening: A rigorous viral panel screens for latent infections, including Cytomegalovirus, Hepatitis, and Human Immunodeficiency Virus, which could lethally reactivate once the immune system is intentionally suppressed.
Reevaluating the Bone Marrow Transplantation Age Limit
Historically, standard medical protocols enforced a strict bone marrow transplantation age limit, typically disqualifying any patient over the chronological age of fifty five due to the insurmountable mortality risks associated with high dose conditioning. However, modern hematological advancements have completely shifted this clinical paradigm.
Today, oncologists prioritize a patient’s physiological performance status over their chronological age. Furthermore, the development of Reduced Intensity Conditioning regimens has revolutionized patient eligibility.
These specialized protocols utilize lower, more tolerable doses of chemotherapy and radiation. Instead of relying entirely on the drugs to physically eradicate the cancer, Reduced Intensity Conditioning suppresses the patient’s immune system just enough to allow the donor cells to successfully engraft.
The medical team then relies heavily on the resulting Graft Versus Tumor effect to destroy the remaining malignancy over time.
Eligibility Stratification Based on Conditioning Protocols
| Transplant Conditioning Regimen | Target Patient Demographic | Primary Clinical Rationale |
| Myeloablative Conditioning (MAC) | Younger patients, typically under the age of sixty, demonstrating optimal baseline organ function. | To maximize immediate cancer eradication utilizing the maximum tolerated doses of systemic toxicity. |
| Reduced Intensity Conditioning (RIC) | Older patients, often up to age seventy five, or those presenting with preexisting clinical comorbidities. | To minimize immediate organ toxicity while successfully leveraging the donor immune system for long term disease control. |
Systematically evaluating the precise physiological status of the patient rather than strictly adhering to outdated chronological restrictions, the hematology team can safely offer this highly curative procedure to a significantly broader demographic of cancer patients.
Why Choose Dasappa Cancer Hospital
The clinical decision to proceed with a hematopoietic stem cell transplant is based entirely on the statistical probability of achieving permanent disease remission.
The long term bone marrow transplantation success rate is highly variable and depends strictly on several specific clinical parameters. These variables include the exact type and stage of the hematological malignancy, the patient’s physiological baseline health, the specific conditioning regimen utilized, and the exact genetic quality of the donor match in allogeneic protocols.
Patients transplanted during their first complete remission statistically demonstrate the highest long term survival rates.
Because this procedure temporarily eradicates the patient’s immune system, achieving these optimal clinical outcomes requires a highly specialized, rigidly controlled medical environment.
Dasappa Cancer Hospital is specifically engineered to support the extreme physiological demands of this intensive therapeutic pathway. Selecting our facility ensures access to the exact clinical infrastructure required for patient survival and long term recovery.
The Dasappa Clinical Advantage
- Multidisciplinary Hematology Board: Every transplant candidate is rigorously evaluated by a collaborative team of surgical oncologists, radiation specialists, and medical hematologists to determine the precise, optimal conditioning regimen.
- Ultra Sterile Isolation Infrastructure: During the profound neutropenic phase following the conditioning chemotherapy, patients are highly vulnerable to opportunistic pathogens. Our facility utilizes dedicated, positive pressure isolation wards equipped with advanced High Efficiency Particulate Air filtration systems to guarantee absolute environmental sterility.
- Comprehensive Post Transplant Management: The critical phase of a transplant occurs in the months following the cellular infusion. Our specialized intensive care teams strictly monitor patients for early signs of infection, organ toxicity, and acute Graft Versus Host Disease, providing immediate pharmacological intervention when medically necessary.
- Integrated Supportive Oncology: We provide continuous nutritional support, targeted pain management, and rigorous psychosocial counseling to assist patients and their families through the extreme physical and emotional exhaustion inherent to the transplant process.
Combining elite clinical expertise with state of the art infrastructural support, Dasappa Cancer Hospital maximizes the statistical probability of a successful cellular engraftment and a complete, long term hematological recovery.
Conclusion
A hematopoietic stem cell transplant represents one of the most complex and intensive medical interventions in modern oncology.
Whether utilizing an autologous protocol to safely administer massive doses of chemotherapy or employing an allogeneic protocol to biologically replace a failing immune system, the procedure requires absolute clinical precision. Patients and families frequently express valid concerns regarding the highly specialized infrastructure required and the resulting bone marrow transplantation cost in india.
At Dasappa Cancer Hospital, our foundational mission is to provide this elite, curative therapy with complete financial transparency and ethical accessibility. We are deeply committed to delivering world class hematological care without compromising our patient first philosophy.
If you or a family member requires an advanced clinical consultation for a blood cancer diagnosis, contact Dasappa Cancer Hospital today to schedule a comprehensive evaluation with our oncology specialists.