When a patient walks into an oncologist’s office, the first question is rarely about the medicine.
It is almost always: “Can Cancer Be Cured?” The short answer is yes.
Millions of people worldwide are living proof that cancer can be eliminated.
According to the National Cancer Institute (NCI), a patient is considered “cured” when there are no traces of cancer after treatment, and the cancer will never come back.
However, the “Long Answer” is more nuanced. In the medical world, doctors are cautious about using the word “Cure” immediately.
Instead, we use the term “Remission” or “No Evidence of Disease (NED).” Why? Because cancer operates at a microscopic level.
Even if a tumor is removed, a single microscopic cell might remain hiding in the body. Therefore, the medical benchmark for a “Cure” is typically the 5-year survival rate.
- The Statistic: If a patient remains disease-free for 5 years after diagnosis, the statistical probability of the cancer returning drops significantly, often to the same level as the general population.
Today, thanks to advancements in Cancer Treatment Types, we are reaching that 5-year mark more often than ever before.
From early-stage breast cancer (which has a 99% survival rate when caught early) to complex blood cancers now treated with Modern Cancer Therapy, the narrative has shifted.
Cancer is no longer a death sentence; for many, it is a treatable condition that can be managed or completely eradicated.
The Medical Dictionary: Cure vs. Remission vs. NED

Decoding the language of your oncologist.
When your treatment ends and you undergo your final PET-CT scan, you might expect the doctor to say, “You are cured.” Instead, they will likely use terms like “Remission” or “NED.” Understanding the clinical difference between Cancer Remission Vs Cure is vital for setting realistic expectations and managing post-treatment anxiety.
Why the hesitation to use the word “Cure”? The answer lies in tumor biology.
Scans can only detect cancer clusters that are a certain size (typically a few millimeters). They cannot detect single, microscopic cancer cells (micro-metastases) that might be floating in the bloodstream.
According to major oncological guidelines, including those from the National Cancer Institute (NCI), here is how we define your Cancer Cure Possibilities at different stages of your journey:
Table: The Clinical States of Cancer Recovery
| Medical Term | Clinical Definition | What It Means For The Patient |
|---|---|---|
| Partial Remission | The cancer has shrunk by at least 50% but is still present. | The treatment is working. The disease is being controlled as a chronic condition, and therapy may continue. |
| Complete Remission (CR) | All signs and symptoms of cancer have disappeared. | Your scans are clear, and tumor markers in your blood are normal. However, you still need regular follow-ups. |
| N.E.D. (No Evidence of Disease) | Often used interchangeably with Complete Remission. The doctor cannot find any physical evidence of cancer. | You have achieved the immediate goal of treatment. You will transition from “active treatment” to “surveillance.” |
| Cured | A state of Complete Remission/NED maintained for a prolonged period (usually 5 years or more). | The statistical probability of the same cancer returning is extremely low. You are considered free of the disease. |
The 5-Year Milestone: Why is it important?
For most solid tumors (like breast, colon, or lung cancer), the risk of recurrence is highest in the first two to three years after treatment.
If the cancer cells were completely eradicated, they obviously cannot grow back. If microscopic cells survive, they usually grow large enough to be detected within that 5-year window.
Therefore, crossing the 5-year mark of Complete Remission is the universally accepted benchmark for declaring a patient “Cured.”
Note: Some slow-growing cancers, like certain types of estrogen-positive breast cancer, may require a 10-year benchmark, while some fast-growing blood cancers can be considered cured much sooner.
What Determines Your Outcome?
Why are some cancers curable while others are chronic?
A common question patients ask is, “My neighbor survived Breast Cancer for 20 years, but my uncle passed away from Pancreatic Cancer in 6 months. Why?”
The answer lies in the biology of the disease. Can Cancer Be Cured? The answer depends heavily on three specific variables that oncologists analyze before starting any Modern Cancer Therapy. Think of this as a “Cure Calculator.”
A. The Tumor Biology
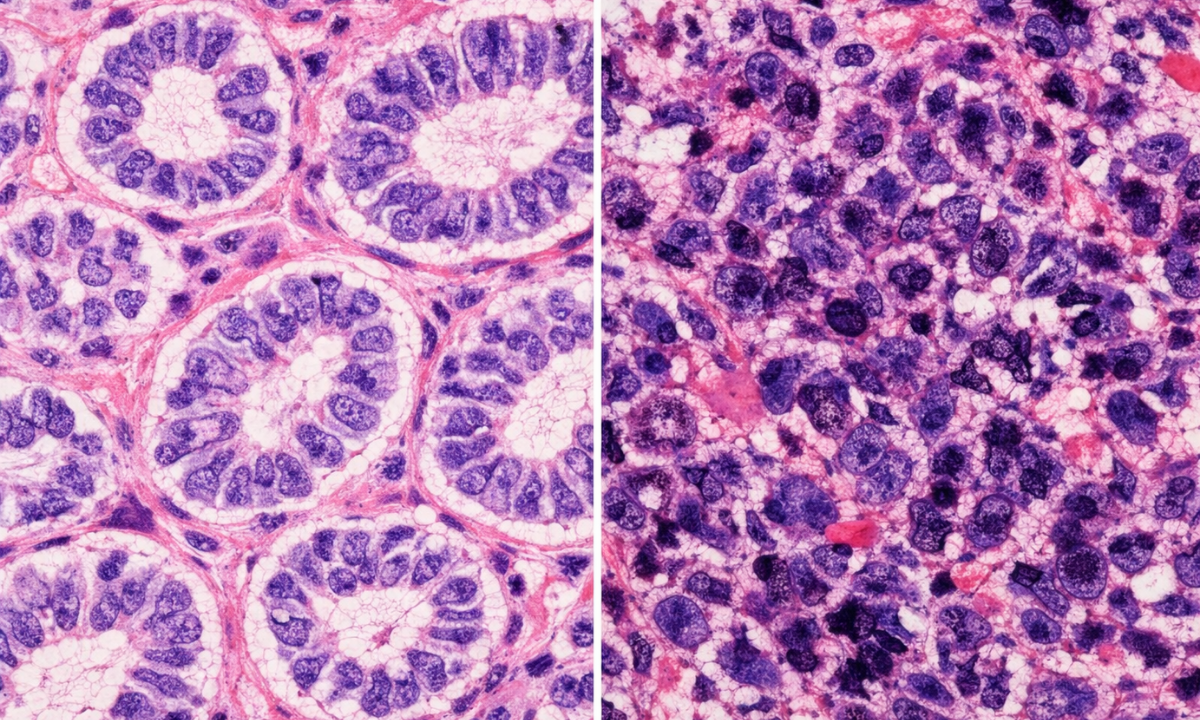
Not all cancer cells behave the same way.
- Low-Grade (Well-Differentiated): These cells look almost like normal cells. They grow slowly and are less likely to spread. Prognosis: Excellent.
- High-Grade (Poorly Differentiated): These cells look wild and disorganized. They divide rapidly and are aggressive. Prognosis: Guarded.
- Example: A low-grade Prostate Cancer might never need treatment, while a high-grade Glioblastoma (Brain Tumor) requires immediate, aggressive intervention.
B. The Stage
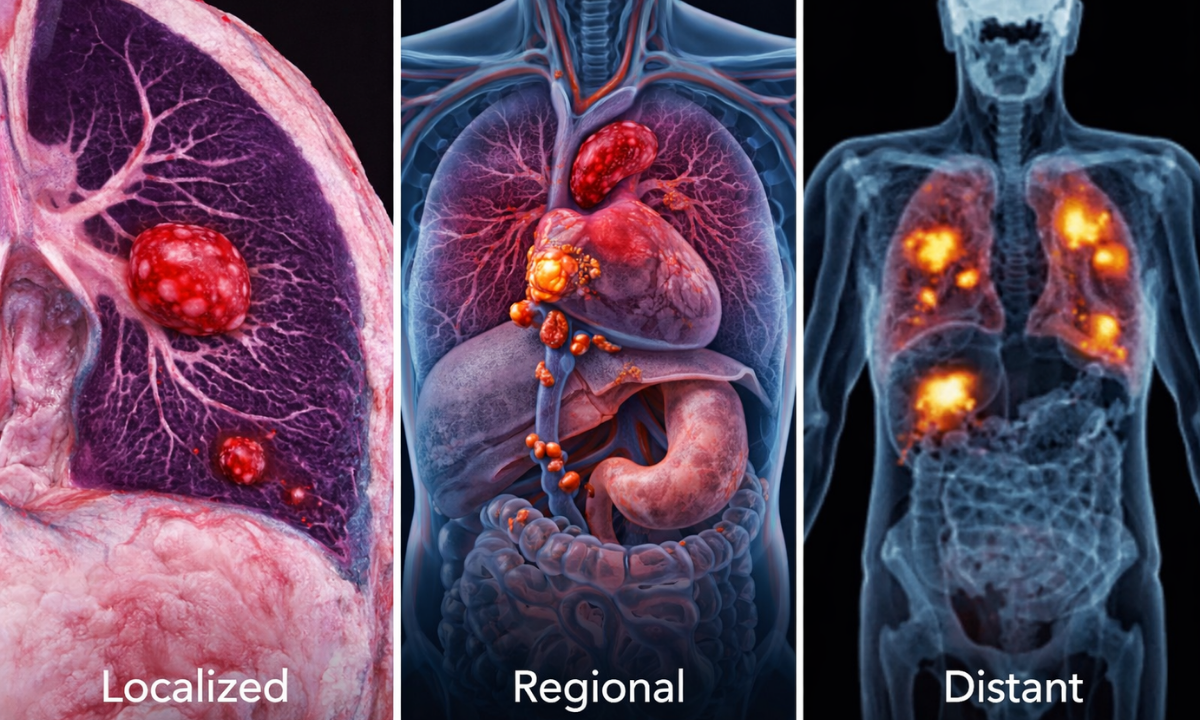
This is the most critical factor in determining Cancer Cure Possibilities.
- Localized (Stage I & II): The cancer is contained in one organ. Cure Rate: High (often >90%).
- Regional (Stage III): The cancer has spread to nearby lymph nodes. Cure Rate: Moderate (requires combination therapy).
- Distant (Stage IV): The cancer has spread to other organs (Metastasis). Cure Rate: Low (Focus shifts to Control/Life Extension).
- Note: Even in Stage IV, “Oligometastasis” (limited spread) are increasingly curable with modern technology.
C. The Molecular Profile
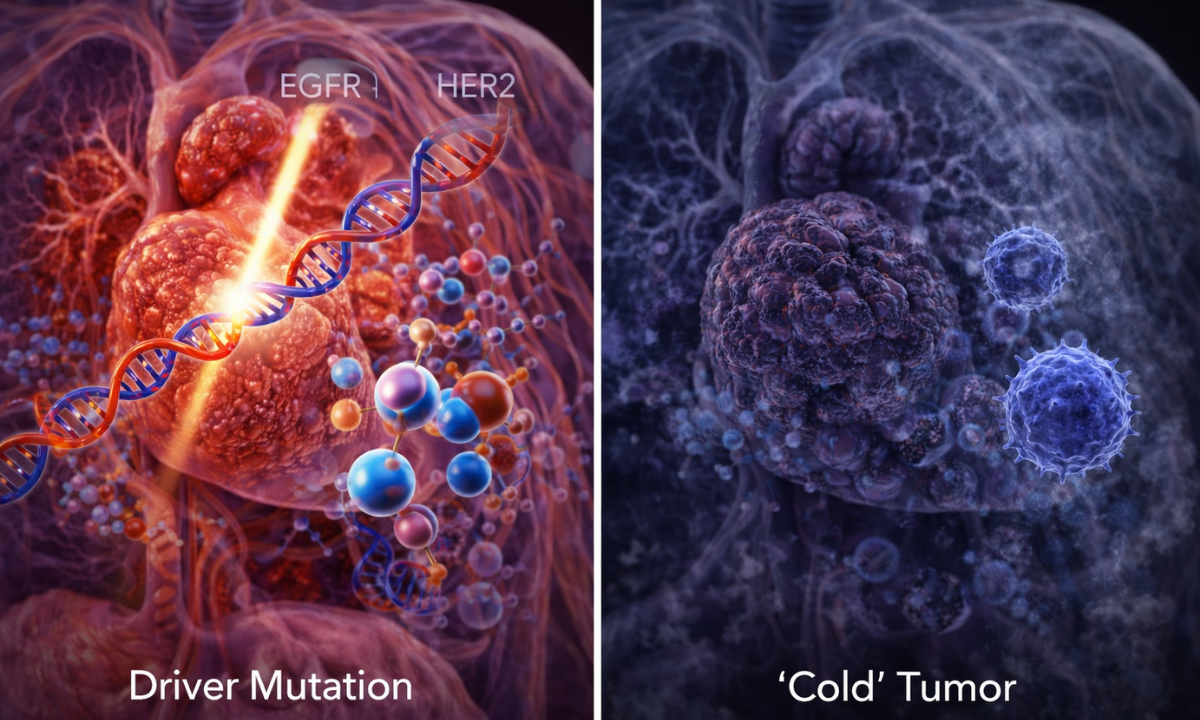
This is the new frontier. Two patients with the same “Lung Cancer” can have completely different outcomes based on their genetics.
- The Driver Mutation: If your cancer has a specific mutation (like EGFR or HER2), we have targeted drugs to shut it down.
- The “Cold” Tumor: If the tumor has no identifiable mutations and hides from the immune system, it is harder to treat.
- Key Insight: Oncological Treatment Options are now tailored to these genes. A patient with a BRCAmutation might be cured with a specific pill (PARP Inhibitor) that wouldn’t work for anyone else.
Table: The Curability Spectrum
| High Cure Potential (>90%) | Moderate Cure Potential (50-80%) | Challenging / Chronic Management (<30%) |
|---|---|---|
| Thyroid Cancer (Papillary) | Colorectal Cancer (Stage III) | Pancreatic Cancer |
| Breast Cancer (Stage I/II) | Cervical Cancer (Early Stage) | Glioblastoma (Brain) |
| Prostate Cancer (Localized) | Kidney Cancer | Lung Cancer (Advanced/Stage IV) |
| Hodgkin Lymphoma | Bladder Cancer | Liver Cancer (Advanced) |
Understanding Cancer Treatment Types
The tools we use to achieve a cure.
A common misconception is that there is a single “Cancer Treatment.” In reality, oncology is a war fought on multiple fronts.
To achieve a Cancer Cure, doctors rarely rely on just one weapon. Instead, we use a Multimodal Approach combining different therapies to attack the cancer from every angle.
We classify these Cancer Treatment Types into two broad categories: Local Therapy (targeting the tumor you can see) and Systemic Therapy (targeting the cells you can’t see).
A. Local Therapy
These treatments are designed to physically remove or destroy the main tumor mass. They are most effective when the cancer is caught early and hasn’t spread.
- Surgery (The “Cold Steel”):
- Goal: Curative Resection (removing the entire tumor with clean margins).
- Modern Twist: We now use Robotic and Laparoscopic Surgery (Keyhole Surgery). This allows us to remove tumors with extreme precision, sparing healthy nerves and organs, which speeds up recovery.
- Radiation Therapy (The “Invisible Beam”):
- Goal: Sterilization. High-energy beams destroy the DNA of any cancer cells left behind after surgery.
- Modern Twist: Technologies like Proton Therapy and CyberKnife allow us to paint radiation onto the tumor with millimeter accuracy, protecting your heart and lungs.
B. Systemic Therapy
This is where the biggest confusion lies. Many patients think “Chemo” is the only option. Today, we have three distinct pillars of drug therapy.
Table: The Three Pillars of Systemic Therapy
| Therapy Type | Mechanism of Action (How it works) | Best For | Key Side Effects |
|---|---|---|---|
| Chemotherapy | It kills all rapidly dividing cells in the body (cancer cells, hair follicles, gut lining). | Aggressive, fast-growing cancers (e.g., Leukemia, Lymphoma, Breast Cancer). | Hair loss, Nausea, Low Immunity. |
| Targeted Therapy | It blocks specific genes or proteins (like EGFR or HER2) that tell the cancer to grow. | Cancers with a specific genetic mutation (e.g., Lung Cancer, Melanoma). | Skin rash, Diarrhea (Usually no hair loss). |
| Immunotherapy | It removes the “mask” cancer uses to hide, training your own immune system to find and kill it. | Advanced cancers that are resistant to chemo (e.g., Kidney, Bladder, Lung). | Fatigue, Auto-immune reactions. |
C. The Hormone Therapy
Some cancers (like Breast and Prostate cancer) use your body’s natural hormones as fuel.
- The Strategy: We don’t poison the cancer; we starve it.
- The Treatment: Pills (like Tamoxifen) or injections block the hormones, effectively cutting off the cancer’s food supply.
The Dasappa Approach: We do not believe in a “copy-paste” protocol. Your treatment plan is designed by our Tumor Board, ensuring you get the exact combination of Oncological Treatment Options whether it’s surgery first, or chemo first that gives you the highest statistical chance of a cure.
The New Era: Immunotherapy, Targeted Therapy, and “Living Drugs”
How we are turning “Terminal” into “Treatable.”
For decades, the answer to “Can Cancer Be Cured?” for Stage IV patients was a definitive “No.”
Today, that answer is shifting to “Possibly” or “It can be managed long-term.” This shift is not due to better chemotherapy, but due to an entirely new understanding of cancer biology.
We have moved from “carpet bombing” the body to “precision engineering.”
Here are the three advancements redefining the word “Cure”:
A. Immunotherapy
Chemotherapy eventually stops working because cancer cells learn how to resist it. The immune system, however, has a “memory.”
- The Mechanism: Cancer cells often survive by putting the immune system to sleep using a “secret handshake” (PD-L1 proteins). Immunotherapy drugs (Checkpoint Inhibitors like Pembrolizumab or Nivolumab) block this handshake, waking up the T-cells to attack the tumor.
- The Evidence (CheckMate 067 Trial): Historically, patients with metastatic Melanoma (skin cancer) had a survival rate of less than 5%.
- The New Reality: Data released in 2024 from the 10-year follow-up of the CheckMate 067 trial showed that nearly 50% of patients treated with dual immunotherapy were still alive a decade later.
- The Verdict: Doctors now call this a “Functional Cure.” The cancer may not be gone, but the immune system keeps it in a permanent “headlock.”
The “Miracle” Case: In a recent study on Rectal Cancer (using the drug Dostarlimab), 100% of patients with a specific genetic mismatch (MMRd) achieved complete remission without surgery or chemo. This is the potential future of Modern Cancer Therapy.
B. Targeted Therapy
For cancers like Lung Cancer or Leukemia, we have moved from IV drips to daily oral tablets.
- The Science: We analyze the tumor’s DNA to find the “Driver Mutation”, the engine running the cancer.
- The Treatment: If you have an EGFR mutation (common in non-smokers with Lung Cancer), you take a pill (Tyrosine Kinase Inhibitor) that shuts off that specific engine.
- The Result: Patients are living for years sometimes decades, treating their cancer exactly like diabetes. It is not “cured” in the sense that they can stop the pill, but they die with the cancer, not from it.
C. CAR T-Cell Therapy: The Living Drug
This is the most advanced form of Oncological Treatment Options available today, primarily for blood cancers.
- How it works: We take your blood, extract your T-cells, and genetically engineer them in a lab to grow “GPS sensors” (Chimeric Antigen Receptors) that detect cancer.
- The Infusion: These super-charged cells are put back into your body. They are “living drugs” that multiply inside you, hunting down cancer cells for years.
- Success Rate: In certain types of Leukemia (ALL) where all other treatments failed, CAR T-Cell therapy has achieved remission rates as high as 80-90%.
Table: Old World vs. New World Treatments
| Feature | Chemotherapy (The Old Way) | Immunotherapy & Targeted (The New Way) |
|---|---|---|
| Target | All rapidly dividing cells (Good & Bad). | Specific mutations or Immune Pathways. |
| Duration | Short bursts (due to toxicity). | Long-term maintenance (Years). |
| Goal | Shrink the tumor temporarily. | Durable Remission or “Functional Cure.” |
| Side Effects | Hair loss, Nausea, and infection risk. | Skin rash, Thyroid issues, Fatigue. |
When Cure Isn’t Possible: Cancer as a Chronic Disease
Redefining what it means to “survive.”
For many patients, hearing the words “It cannot be cured” sounds like a final verdict. But in modern oncology, “Incurable” does not mean “Untreatable,” and it certainly does not mean “Terminal.”
We are witnessing a massive paradigm shift where Advanced Cancer is increasingly being treated as a Chronic Non-Communicable Disease (NCD). To understand this, look at Diabetes or Hypertension.
- The Parallel: You cannot “cure” diabetes. The pancreas will not fix itself. However, with daily insulin and lifestyle changes, a diabetic patient lives a full, normal lifespan.
- The Cancer Reality: Today, we treat many metastatic cancers (like Breast, Prostate, and CML Leukemia) with the same philosophy. The goal shifts from eradicating the disease to managing it.
A. The New Goal: Progression-Free Survival (PFS)
When a cure is no longer the objective, the medical goal changes to Progression-Free Survival. This means keeping the cancer “stable” (not growing) for as long as possible while ensuring you feel good.
- Stable Disease: You might live with a tumor in your body for 10 years. As long as it doesn’t grow or spread, you are “winning.”
- Maintenance Therapy: Instead of high-dose chemo that keeps you in bed, you might switch to “Maintenance Therapy”, often a low-dose pill or a monthly injection that keeps the cancer asleep with minimal side effects.
B. The Strategy
Think of your treatment plan not as a single shot, but as a game of chess. We use treatments in a specific sequence, called Lines of Therapy.
- First-Line Therapy: The best, most effective drug we use first. It might work for 2 years, 5 years, or longer.
- Second-Line Therapy: If the cancer learns to resist the first drug, we don’t give up. We switch to the “Second Line”, a different drug with a different mechanism of action.
- Third-Line & Beyond: We continue to swap weapons. With the speed of modern research, by the time you need a Third-Line drug, a new one might have just been invented.
C. The Gap
This is a concept that surprises many patients. If your scans show Stable Disease for a long time, your Best cancer treatment hospital in Bangalore might suggest a “Drug Holiday.”
- What it is: A planned break from all treatment.
- The Goal: To let your body recover, wash out toxins, and allow you to travel, attend weddings, or just feel “normal” again. We monitor you closely, and if the cancer wakes up, we restart the treatment.
Table: Acute vs. Chronic Treatment Mindset
| Feature | Curative Approach (Acute) | Chronic Management Approach |
|---|---|---|
| The Goal | Kill every single cancer cell immediately. | Keep the cancer stable; prevent growth. |
| The Intensity | Maximum tolerated dose (High Toxicity). | Minimum effective dose (Low Toxicity). |
| The Duration | Short-term (e.g., 6 months of Chemo). | Indefinite (Years of Maintenance). |
| Success Metric | “Cancer-Free” (Complete Remission). | “Living Well” (Quality of Life). |
Conclusion
The question, “Can Cancer Be Cured?” is no longer a simple yes or no. It is a spectrum. For some, it means a complete surgical cure and walking away forever.
For others, it means a “Functional Cure” through Immunotherapy, where the body keeps the disease in check for decades. Many with advanced disease, it means turning cancer into a chronic, manageable companion, allowing you to watch your children graduate, and your grandchildren grow.
The Most Important Variable: Your Care Team. While we cannot always control the biology of the tumor, we can control the quality of the fight.
Navigating the complex world of Cancer Treatment Types, from deciding between surgery and radiation to accessing the latest clinical trials, requires more than just a doctor.
It requires a Multidisciplinary Tumor Board.
At Dasappa Cancer Hospital, your life is never left to a single opinion. Our board of surgeons, medical oncologists, and pathologists reviews every case together, ensuring you receive a Precision Treatment Plan tailored to your specific genetic profile.
Do Not Wait.
Whether you are seeking a primary diagnosis or a second opinion on a difficult case, the right strategy can change the outcome.
If you are looking for the Best cancer treatment hospital in Bangalore that combines cutting-edge Modern Cancer Therapy with compassionate care, we are here to fight alongside you.